Quitting vaping: what science tells us
Among young adults, some interventions do seem to raise quit rates.

The evidence on helping young adults quit is improving. It is still thinner than it should be.
For years vaping was treated as either a moral panic or a neat off-ramp from smoking. Neither view was especially useful.[1][4] The first ignored the fact that many young users are heavily dependent on nicotine. The second often assumed that quitting vaping would look much like quitting cigarettes. The literature now suggests a less tidy picture.[2][4][6]
Among young adults, some interventions do seem to raise quit rates.[2][3][4] Digital support helps, especially when it is built for the habits of younger users rather than copied from older smoking-cessation campaigns.[2][3] Medication also helps, above all for people with stronger nicotine dependence.[2][4][6] The best results appear to come when behavioural support and pharmacological treatment are used together.[2][4]
That is the encouraging part. The discouraging part is that much of the research remains short-term, uneven and, in some corners, too close to industry money.[1][4] Clinical guidance tailored specifically to vaping is still underdeveloped.[4][6] The market has moved faster than the science.
What works
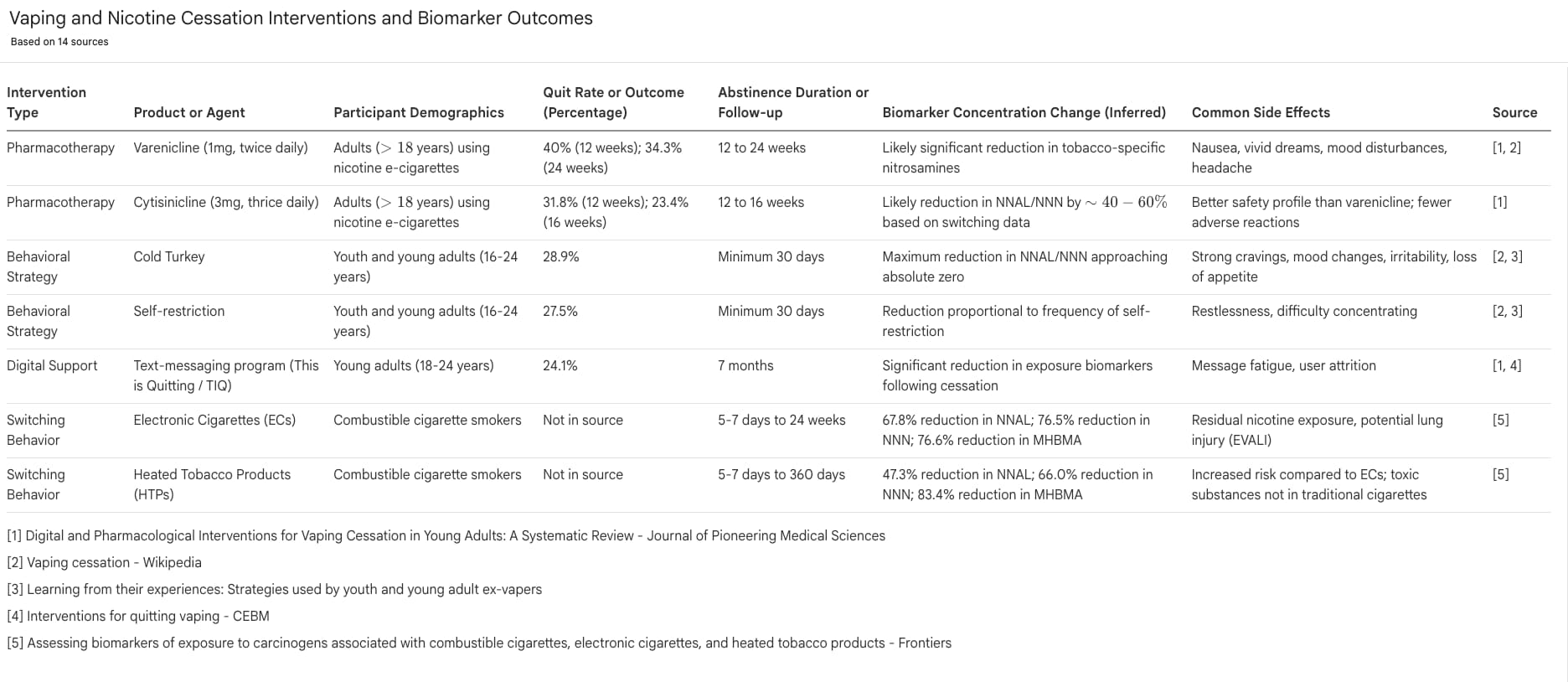
The clearest behavioural evidence in this literature comes from digital interventions, especially text-message programmes aimed at younger users.[2][3] The best-known example is “This is Quitting”, a tailored mobile programme tested in young adults.[2][3] In the study cited in your source set, abstinence at seven months reached 24.1% in the intervention group, compared with 18.6% in the control group.[2] That is not a spectacular number. It is, however, a real improvement delivered through a cheap and scalable format.[2][3]
That matters because vaping is not merely a chemical habit. It is also woven into boredom, stress, routine and social life.[5] A phone-based intervention has an obvious advantage in such a setting: it reaches users in the same place where cravings, cues and poor decisions often arise.[2][3] Secondary analysis of the same programme also suggested that a nicotine-focused intervention could improve abstinence from cannabis as well.[3] That does not make texting a cure-all. It does make it one of the more plausible tools on offer.[2][3][4]
Medication appears to be the other bright spot.[2][4][6] Reviews in your source set point in particular to varenicline and cytisinicline.[2][4] In one varenicline trial, continuous abstinence at 12 weeks reached 40%, compared with 20% on placebo, with a gap that remained visible at 24 weeks.[2] In the ORCA-V1 trial, cytisinicline produced a 31.8% abstinence rate at 12 weeks, against 15.1% for placebo.[2] The studies differ in design, so the figures should not be treated as directly comparable. Even so, they point in the same direction: medicine can improve the odds of quitting, especially for heavier users.[2][4]
The larger lesson is that vaping cessation probably works best when treated as both a physiological and a behavioural problem.[2][4] Medication can reduce withdrawal and craving.[2][6] Behavioural support can help users handle triggers, routines and relapse.[2][4][5] This is not a glamorous insight. It is merely the one most consistent with the evidence.
What does not work
What looks weakest is the assumption that vaping can simply be folded into the old smoking-cessation script.[4][6] In practice, much care still borrows from smoking protocols and adapts them on the fly.[4][6] That is understandable. It is also unsatisfactory. Vapes differ from cigarettes in ways that matter to treatment: nicotine delivery can be faster, doses can be higher, flavours can make repeated use easier, and the device itself can become part of the habit loop.[4]
This helps explain why standard nicotine-replacement approaches may not always be enough.[4][6] A user taking in large amounts of nicotine through a modern vape may find conventional dosing too weak to suppress cravings.[4] That does not mean nicotine replacement has no role. It means that treating vaping as a mere copy of smoking may lead clinicians to under-treat dependence.[4][6]
Unsupported quitting is also common, but the literature does not suggest it is the most reliable route.[5] In the qualitative study of youth and young adult ex-vapers, “cold turkey” and self-restriction were among the most commonly reported strategies.[5] Some participants succeeded that way. Many also described relapse driven by social influence, mood and circumstance.[5] A popular method is not necessarily an effective one. Sometimes it is simply the easiest method to attempt with no help at hand.
The biomarker literature deserves special caution.[1] One of the stronger accessible sources in your list is a 2025 systematic review and meta-analysis of 18 randomised trials on biomarkers of exposure among people who switched from combustible cigarettes to e-cigarettes or heated tobacco products.[1] It found lower exposure to several carcinogens among switchers, at times approaching the levels seen in abstainers.[1] That is an important result. But most of the included studies were industry-funded and most followed participants only briefly.[1] A short-term fall in biomarkers is useful evidence. It is not the same thing as a settled verdict on long-term safety.
What still needs to be known
The biggest gap is the lack of proper clinical guidance designed specifically for vaping cessation.[4][6] A 2021 health-technology review found little in the way of evidence-based pharmacological guidance for vaping.[6] More recent reviews show that the evidence base is improving, but not yet mature.[2][4] Too much current practice still amounts to borrowing from smoking medicine and hoping the fit is good enough.[4][6] It often is not.
Longer follow-up is another obvious need.[1][2][4] Many studies measure abstinence after weeks or a few months.[1][2] That is enough to show whether a treatment can get users started. It is not enough to show whether they stay quit. Relapse is not a side issue here; it is the central issue.[4][5] A treatment that performs well at 12 weeks but fades by 12 months may still be useful, but it tells a different story from one that produces durable abstinence.
The literature also needs to get more specific about who is quitting, and under what conditions.[2][5] Young adults are not a single block. Some vape heavily; some use nicotine and cannabis together; some are driven chiefly by stress; others by social setting.[3][5] The qualitative evidence in your source set suggests that social influences are an especially important relapse trigger for some groups, including female participants in one study.[5] Device type, flavour, nicotine concentration and patterns of dual use probably matter too.[2][4] These should not be treated as afterthoughts. They may determine which intervention works for whom.
A final problem is the shape of the evidence itself. Several potentially useful papers in your list were inaccessible because of captchas, security checks or other technical barriers. That does not invalidate the accessible sources. It does mean the published picture is still being viewed through a narrower window than one would like. On the material that is accessible, though, the broad conclusion is plain enough: text-based behavioural support helps; medication can help more when dependence is strong; and a combined approach looks the most sensible.[2][3][4][5][6]
Young adults can quit vaping. The evidence says so.[2][4][5] But the field is still at an awkward stage. There is enough research to reject fatalism. There is not yet enough to claim mastery.
Sources
[1] “Assessing biomarkers of exposure to carcinogens associated with combustible cigarettes, electronic cigarettes, and heated tobacco products - Frontiers” (2025). Systematic review and meta-analysis of 18 randomised controlled trials on biomarker exposure after switching from combustible cigarettes to e-cigarettes or heated tobacco products.
[2] “Digital and Pharmacological Interventions for Vaping Cessation in Young Adults: A Systematic Review - Journal of Pioneering Medical Sciences” (2025). Review of text-messaging programmes and medications such as varenicline and cytisinicline for ages 18–24.
[3] “Groundbreaking Study Reveals Text Message Vaping Cessation Program Also Helps Young People Quit Cannabis - Truth Initiative” (2025). Summary of secondary analyses showing that the “This is Quitting” intervention also improved cannabis abstinence.
[4] “Interventions for quitting vaping - CEBM” (2025). Briefing based on a Cochrane living systematic review of behavioural and pharmacological interventions.
[5] “Learning from their experiences: Strategies used by youth and young adult ex-vapers” (2023). Qualitative study on cessation strategies and relapse triggers among former vapers in Canada.
[6] “Pharmacological Interventions for Vaping Cessation - NCBI Bookshelf - NIH” (2021). Health-technology review noting the lack of evidence-based pharmacological guidelines specific to vaping cessation.